
MCHC
The MCHC (mean corpuscular hemoglobin concentration) is the mean hemoglobin concentration or content of hemoglobin per unit volume (weight/volume or g/dL) in red blood cells (RBC). Alternatively, it can be thought of the percentage of the RBC that consists of hemoglobin. It is a calculated value, obtained by dividing the hemoglobin, as measured spectrophotometrically after RBC lysis in the instrument, by the RBC mass as determined by the HCT or PCV.
MCHC (g/dL) = (Hgb ÷ PCV) x 100
or
MCHC (g/dL) = (Hgb ÷ HCT) x 100
The HCT is a calculated result itself, so you can use the primary components of the HCT to rearrange the above formula to:
MCHC (g/dL) = (Hgb ÷ [MCV x RBC count]) x 100
Unlike the MCH, this measurement does take into account the volume of the RBC and represents the average concentration (weight/unit volume) of hemoglobin in RBCs. When the HCT is used for the calculation, it will be influenced by changes in the MCV and RBC count (see formula above). In an animal with a regenerative anemia with numerous polychromatophilic RBCs that are larger than normal (increased MCV) but contain less hemoglobin than normal (because they are immature), the MCV and MCH will track high together (MCH being dictated by the larger cell volume), whereas the MCHC will reflect the true low hemoglobin concentration in the cells (tracking low). Similarly, in an animal with small RBCs and a low MCV, a low MCH may reflect smaller RBCs with normal hemoglobin or less hemoglobin. A normal MCHC would reflect smaller cells with normal hemoglobin whereas a low MCHC would reflect smaller cells with less hemoglobin. The latter is often seen in iron deficiency anemia.
CHCM
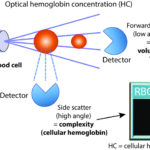
The ADVIA hematology analyzer also provides a CHCM, which is the mean of the optically measured hemoglobin concentration within the cells, i.e. per unit volume (g/dL), and, like the MCHC, takes into account the volume of the cell. With the CHCM, instead of the hemoglobin being measured spectrophotometrically after the RBCs are lysed, the hemoglobin content only within intact RBCs is optically measured based on the degree of laser light the RBCs scatter in a side direction (high angle light scatter, also called internal complexity) as they pass in single file through a laser beam in a flow cell. The cell volume is also simultaneously measured by the degree of forward (low angle) scatter (see image to the right) and the hemoglobin content per cell is converted to a concentration (content per unit volume). The CHCM can be considered the optical equivalent of the MCHC of intact RBCs. This measurement cannot be done on RBCs that have lysed.
Thus, for every blood sample we run, we obtain a calculated MCHC (from measured hemoglobin after lysing RBC) and an optically or directly measured CHCM (from internal complexity of intact RBC), both in g/dL and both equivalent to the hemoglobin concentration or hemoglobin content per volume. We usually only report the MCHC, but in some cases we provide the CHCM and a total hemoglobin concentration calculated from the CHCM, mean cell volume and RBC count (calculated hemoglobin = [CHCM x MCV x RBC] ÷ 1000). This is particularly used with lipemic samples in which lipemia falsely increases the spectrophotometrically measured hemoglobin concentration, but has no effect on the HCT or RBC count, resulting in a falsely increased MCHC (and MCH). In these situations, we delete the measured hemoglobin concentration (as it is falsely high) and the related indices dependent on that hemoglobin concentration, MCH and MCHC, and provide results for a calculated hemoglobin concentration, CH and CHCM, which are all obtained from the light scatter of intact RBC, since the scatter of the laser light is not affected by the lipid particles.
RBC hemoglobin indices summary
This is summarized below.
- MCHC (mean corpuscular hemoglobin concentration): This is calculated from a direct spectrophotometrically measured hemoglobin after lysis of RBCS within the analyzer and is the RBC index that is provided on our routine hemograms for most species (exotic species are an exception). Since it is a calculated value, dependent on the hemoglobin concentration and HCT (MCV and RBC count), false increases or decreases in any of these results will falsely change the MCHC.
- CHCM (cellular hemoglobin concentration mean): CHCM is the mean of a direct optically measured hemoglobin from the hemoglobin content and volume of intact RBCS as they pass through a laser light. This is used to back-calculate a calculated or cellular hemoglobin concentration from all intact RBCs as shown above. It is affected by fewer artifacts than the spectrophotometrically measured hemoglobin concentration and we provide this value (with the calculated hemoglobin concentration and mean hemoglobin content or CH) when the spectrophotometrically measured hemoglobin concentration is inaccurate, e.g. lipemia, and other settings where the RBC count is proportionally lower than the spectrophotometric measured hemoglobin concentration (in vitro or in vivo hemolysis, agglutination).
| Result | Derivation | Details | Reported |
| Hemoglobin or Hgb concentration (g/dL) in all RBCs | Direct measurement | RBC are lysed in the machine and all the hemoglobin is measured at a specific wavelength (540 nm) using spectrophotometry | Routine hemogram, except if lipemia falsely increases. Does not accurately reflect oxygen-carrying capacity with true in vivo intravascular hemolysis but does with in vitro hemolysis |
| MCH (pg) = mean hemoglobin content | Calculated from the directly measured hemoglobin above | (Hgb x 10) ÷ RBC | Routine hemogram, unless falsely increased (e.g. lipemia, agglutination, in vivo intravascular or in vitro hemolysis) |
| MCHC (g/dL) = mean hemoglobin concentration | Calculated from the directly measured hemoglobin above | (Hgb ÷ PCV) x 100 (Hgb ÷ HCT) x 100 or (Hgb ÷ [MCV x RBC count]) x 100 |
see MCH |
| Calculated or cellular hemoglobin concentration (g/dL) of all intact RBCs | Calculated from the optically measured hemoglobin concentration, red blood cell count and cell volume | (CHCM x MCV x RBC count) ÷ 1000 or (CH x RBC count) ÷ 10 (content per RBC x # RBC) |
Not on routine hemograms, unless measured hemoglobin inaccurate or disproportionate to RBC count (see above) |
| CH (pg) = mean optical hemoglobin content of intact RBCs | Direct optical measurement (intact RBC only) | From internal complexity of each intact RBC by side scattered (low angle) laser light, which is then averaged | Not on routine hemograms, unless MCH inaccurate (see above) |
| CHCM (g/dL) = mean optical hemoglobin concentration of intact RBCs | Direct optical measurement (intact RBC only) | Hemoglobin content (side scatter) ÷ volume (forward scatter) of each individual RBC, which is then averaged | Not on routine hemograms, unless MCHC inaccurate (see above) |
Units of measurement
MCHC and CHCM are measured in g/dL (conventional units) or g/L (SI units). The conversion formula is as follows:
g/dL x 10 = g/L
Sample considerations
Sample type
Whole blood
Anticoagulant
EDTA is the preferred anticoagulant.
Stability
The MCHC is unstable. It can either decrease (storage-associated RBC swelling, which increases the MCV) or increase if there is RBC lysis in vitro with storage.
Interferences
- Lipemia: Will falsely increase MCHC due to false increases in measured hemoglobin. It will have no effect on the CHCM.
- Hemolysis: In vivo intravascular hemolysis or in vitro (artifactual) hemolysis falsely increase the MCHC (measured hemoglobin is proportionally higher than HCT or PCV) and decrease the calculated hemoglobin and thus the CHCM (because there are fewer intact RBC – this will be a false decrease with in vitro but not in vivo intravascular hemolysis).
- Icterus: No effect.
- Other:
- Heinz bodies (many, particularly if large) may falsely increase the MCHC (Dondi et al 2019), with less of an effect on the CHCM (personal observations).
- Agglutination: Falsely increases the MCHC (measured hemoglobin is proportionally higher than HCT) with newer optical-based analyzer. The CHCM is more accurate in this setting.
- Excess EDTA: This dehydrates RBC, falsely increasing the MCHC and CHCM.
Test interpretation
Increased values (hyperchromic)
- Artifact:
- MCHC: This is always an artifact because RBCs cannot contain more hemoglobin than normal. This is most frequently due to lipemia, but can also be seen with large numbers of (typically large) Heinz bodies (>50% in cats), hemolysis (in vitro or in vivo intravascular), RBC nuclei (many nRBC), and agglutination. Other causes of a high MCHC is RBC dehydration if there is excess EDTA for the amount of blood in the sample (EDTA dehydrates RBC) or hypo-osmolality – in the latter cases, the high MCHC can be accompanied by a lower MCV (MCV will be lower than it “should be” even if not below the reference interval).
- CHCM: Excess EDTA or hyponatremia.
Decreased values (hypochromic)
- Artifact:
- MCHC/CHCM: RBC swelling with storage and causes of hyperosmolality such as hypernatremia and hyperglycemia (see MCV). This is the most common cause of a low MCHC and is usually seen with an increased MCV (may not always be above the reference interval). The CHCM will also be low in this setting.
- Pathophysiologic:
- Regenerative anemia: Immature RBC have less hemoglobin than normal. This is not a consistent finding in regenerative anemia. Remember, changes require that most of the RBC have less hemoglobin to shift the mean value below the lower reference limit. Red blood cells do not appear hypochromic on a blood smear (they appear to have normal hemoglobin content visually on blood smear examination.
- Iron deficiency anemia: Multiple causes. RBC may be hypochromic on smear examination (contain less hemoglobin which leads to increased central pallor). Animals with iron deficiency are usually anemic by the time the MCHC is decreased. Thus hypochromasia (low MCHC) in the absence of anemia should not be automatically attributed to iron deficiency. However hypochromic RBCs (cells that contain less hemoglobin than normal) may be evident in a blood smear before the MCHC is decreased (but are usually only seen if the animal is anemic).
- Portosystemic shunts: The low MCHC is attributable to a relative or functional iron deficiency (iron is sequestered in the body versus truly deficient). Most animals with low MCHC from shunts usually are truly iron deficient (from concurrent gastrointestinal bleeding).
- Decreased hemoglobin production: Lead poisoning, vitamin B6 deficiency, copper deficiency. These are very uncommon causes of a low MCHC.
- Pathologic causes of RBC swelling: RBC membrane changes, e.g. hereditary stomatocytosis. Alterations in DNA metabolism do not usually result in low MCHC.