
Cerebrospinal fluid from a cat
Case information
A 10-year old-male castrated Domestic Shorthair cat presented to the Cornell University Hospital for Animals (CUHA) Emergency Service for a one-week history of collapsing episodes, as well as lethargy and decreased appetite of one month’s duration. Each episode occurred after the cat rose from bed and lasted 3-4 seconds, during which the cat would become stiff and fall down. The cat did not urinate or defecate during the episodes. No clinical signs were observed before or after the episodes. Based on the owner’s description and an unremarkable neurologic examination other than bilateral mydriasis, seizures were determined to be unlikely, and the cat was transferred to the Cardiology Service for a diagnostic work-up of presumed syncopal episodes.
An electrocardiogram (ECG) and echocardiogram were performed and unremarkable. The patient was sent home with a 24-hour Holter monitor, which recorded a brief period of mild bradycardia (100 bpm) during a collapse episode, however the heart rate was not considered low enough to cause syncope in a cat. No other significant arrhythmias or abnormalities were noted. Bloodwork abnormalities included a marked increase in creatine kinase (CK) activity (17,589 U/L, reference interval [RI], 73-388 U/L) and a moderately increased cardiac troponin concentration (1.39 ng/mL, RI 0.0-0.09 ng/mL). Both analytes were rechecked two days later; the CK activity had markedly decreased to 1,263 U/L and the troponin concentration had decreased, but was also still moderately elevated at 0.73 ng/mL. A consultation with the Neurology Service did not identify any major abnormalities, aside from bilateral mydriasis and possibly an abnormal gait in the pelvic limbs. The Ophthalmology Service performed a fundic examination and diagnosed bilateral chorioretinitis and posterior incipient cataracts.
The Internal Medicine Service was then consulted. Based on the increased CK activity and chorioretinitis, the leading differential diagnosis was toxoplasmosis. A serum sample was submitted for Toxoplasma gondii IgG and IgM antibody titers, and the cat was started on an empiric course of clindamycin. The episodes continued despite this treatment and titer results were negative for the presence of IgM antibodies. However, IgG antibodies were detected, suggesting previous exposure, but not an active infection.
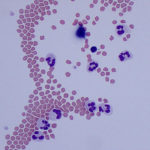
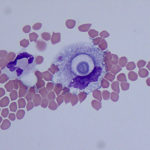
The cat was presented again to the CUHA Neurology Service three weeks later. The neurologic exam was now markedly abnormal with an obtunded mentation, right head tilt, vestibular ataxia, decreased tactile placing in the left thoracic limb, and pain on palpation of the neck and head. In addition, excessive sneezing was reported. Neurolocalization based on these signs diagnosed a left-sided paradoxical cerebellovestibular lesion. Bloodwork was unremarkable other than a persistently increased cardiac troponin concentration (0.64 ng/mL), but a repeat echocardiogram and electrocardiogram remained within normal limits. Magnetic resonance imaging (MRI) was then performed to further work-up the cat’s neurologic disease. Hyperintensity in the area of the cerebellum and midbrain was evident on T1-post contrast MRI, suggestive of infectious or inflammatory cerebellitis. An atlanto-occipital cerebrospinal fluid (CSF) tap was then performed and submitted for cytologic evaluation. The nucleated and red blood cell (RBC) counts of the CSF were 113 cells/μL and 3,714 cells/μL, respectively. The total protein was 29 mg/dL.
Evaluate the provided representative images and answer the following questions:
- How would you classify the inflammation?
- Can you identify the cause of the inflammation?
- What is the likely cause of the increased number of RBCs in the sample?
|
|
|
|

Answer on next page