
Fine needle aspirate of an enlarged jejunal lymph node from a cat
Case information
A 3 year old male castrated domestic shorthair cat presented to the Cornell University Hospital for Animals (CUHA) for an approximately one month history of lethargy, inappetence, and weight loss, and a 4 day history of malodorous urine. Prior to presentation at CUHA, the owners brought the cat to their primary care veterinarian who performed a urinalysis, which was reportedly suggestive of a urinary tract infection. Clavamox was empirically prescribed pending urine culture results. There was no bacterial growth on the culture, therefore the Clavamox was discontinued after 3 doses.
The cat was being managed by CUHA’s Internal Medicine service for pure red cell aplasia (PRCA; see Case of the Month January 2015), which was diagnosed 11 months prior. The cat had developed anemia-induced cardiomyopathy and congestive heart failure that required management with cardiac medications for six months. The PRCA had gone into remission 3 months after the initial diagnosis with a treatment regimen of prednisolone and cyclosporine. The prednisolone therapy induced diabetes mellitus, which was reversed with steroid tapering and prescription diet management. A month prior to the current visit, a recheck packed cell volume at the primary care veterinarian was stable at 35%, and the prednisolone dose was further tapered. Shortly thereafter, the owners noticed the lethargy and inappetence. The cat was an indoor cat, but allowed to go outside in an enclosure. The cat had been seen holding a chipmunk in the mouth a couple of weeks prior to presentation.
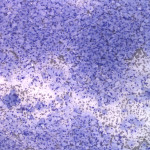
On presentation, the cat was bright, alert, and responsive, and vital signs were within normal limits. Physical examination was unremarkable with the exception of a grade 1/6 left parasternal heart murmur. Due to the history of malodorous urine, a urinary tract ultrasonographic examination was initiated, which was extended to include the entire abdomen due to the identification of enlarged jejunal lymph nodes. The cat was sedated for fine needle aspiration of the jejunal lymph nodes. Squash preparation smears were prepared and submitted for cytologic evaluation.
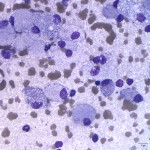
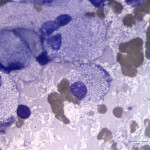
Representative Wright’s stained images are present below. After examining the images, answer the following questions:
- What is the predominant cell type present? Is this an expected finding for a lymph node aspirate?
- What is within the cytoplasm of the cells, as well as extracellularly in the background of the smear?
- What are predisposing factors for your diagnosis based on the patient’s clinical history?
|
|
|
|
Answers on next page